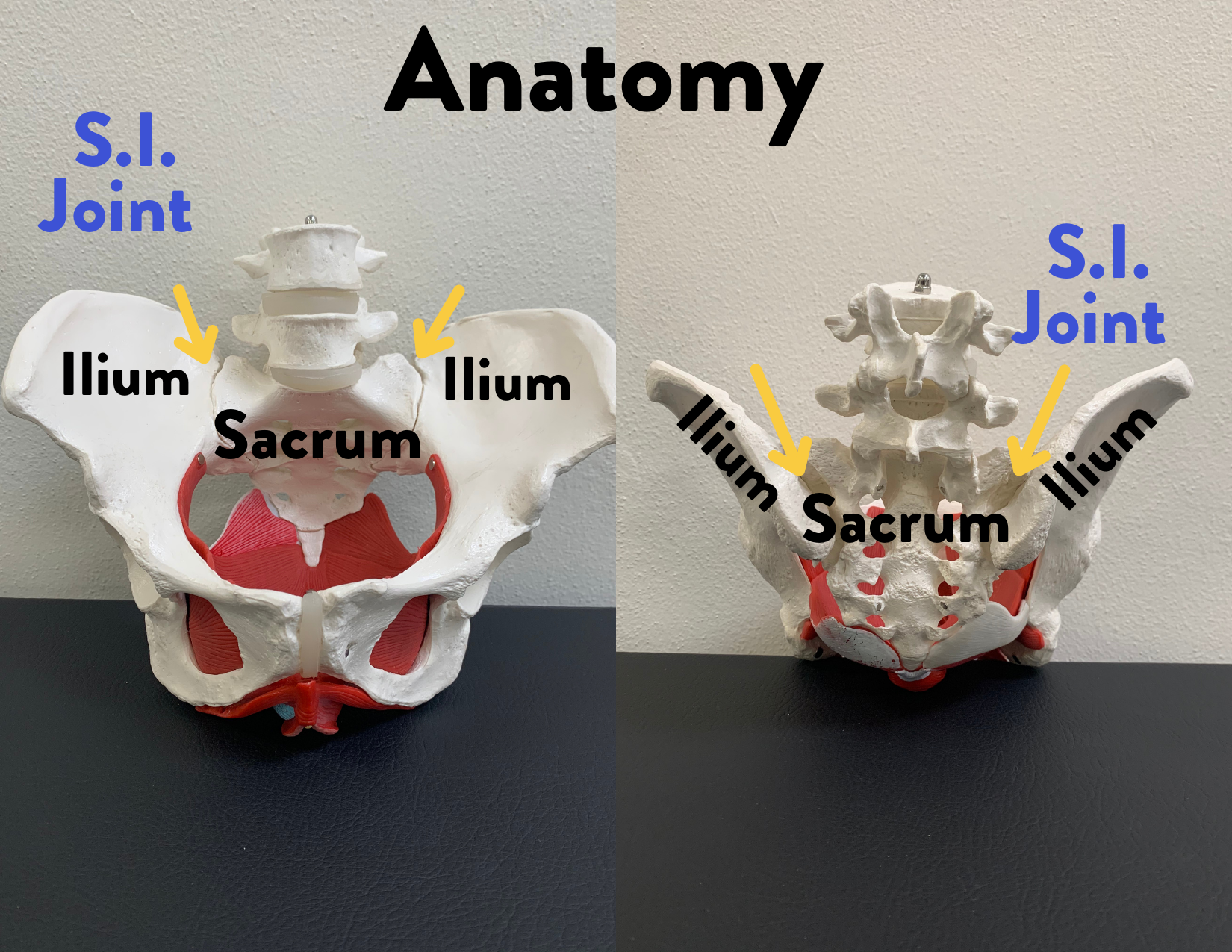
Where is the S.I. joint? What is made up of?
The S.I. Joint is located on either side of the pelvis. It is the contact between the sacrum and the ilium. The sacrum is a triangular shaped bone that sits at the very bottom of your low back and the ilium is the flared or “elephant ear” shape of your pelvis. The joint is stabilized by both passive and active structures that help keep it healthy and secure. Passive structures like the joint capsule and robust network of strong ligaments act as an anchor for the joint to connect the sacrum to the ilium. But the tricky part about this joint is that it has an intricate network of nerves that supply this joint which plays a big role in how patients experience pain especially when they have dysfunctions here. Active structures like muscle cross over the joint to help further stabilize the joint, these are the things we have more control over.
The S.I. joint is a relatively stable joint, it has some mobility that it is responsible for but its main function is to be a secure point of stable load transfer as forces move from the spine down or from the legs up.
The S.I. joint never works alone, it is part of a larger system that has to work together constantly to keep you moving efficiently and be pain-free!. When considering the proximity of the S.I. joint to the low back, pelvic floor and hip, it’s easy to see that these structures frequently have to coordinate and share the work of daily activities. We call this concept regional interdependence and when one teammate is dysfunctional it can have an impact on the whole system. This not only goes for the S.I. joint affecting other areas but also the other areas affecting the S.I. joint. We want to see every part chipping in their effort to help us move, live and exercise as best we can.
What is S.I. Joint Dysfunction?
S.I. joint dysfunction is a condition where the 2 surfaces, the sacrum and the ilium, are either experiencing too much motion or too little motion and this starts to produce pain. This change interrupts its load transfer capabilities therefore the distribution of load is not equal. It is hypothesized that patients experience pain like this due to the fact that the S.I. is reinforced with so many nerve structures. In addition, dysfunction in this area is rarely an isolated event and usually comes with a sequence of impairments in other areas, specifically the lumbar spine, pelvic floor and the hips. Patients will commonly experience one or more of the following symptoms.
There are typically many specific activities that will increase pain
Why do people develop S.I. dysfunction?
This issue is seen frequently in the pregnant and postpartum population due to hormonal changes experienced with pregnancy that have an effect on your joints as they become more lax to prepare for delivery. It can also be further irritated by the postural changes that stresses the body as the baby grows. While prevalent in the pregnant population, it is not limited to that population alone. This can be caused by significant asymmetries in your hip and core muscle strength from left to right or an offset injury that was experienced on one side like misstepping off of a curb. It could also be due joint changes that we experience with aging like degenerative or arthritic changes in the joint.
Presence of joint degeneration does not doom you to being in pain for the rest of your life. Studies like this one here show us that many people walk around with S.I. joint degeneration and don’t even know it!
Who can help you with it?
Self Management
Ways to manage it on your own include daily habits changes, exercises and stretches that can have a big effect on your pain.
Here are some tips on how to manage it yourself.
Chiropractic Care
Chiropractic care can be a helpful tool to manage the pain severity. Their adjustments give a reset to your neuromuscular system which reduces pain and helps improve your movement.
Physical Therapy
We might be biased but physical therapy is the best first line of defense in helping you manage S.I. joint pain. It also pairs really well with chiropractic care too because adjustments are really helpful for joint positioning but we then have to train those muscles how to maintain that position so the problem does not perpetuate. Physical therapists can help identify areas of dysfunction that are creating or contributing to the problem, help you learn movement patterns that will reduce pain with your day to day activities and give you an exercise program to work on your impairments. Interventions usually include a variety of approaches including manual therapy, exercises interventions and other techniques like use of S.I. belt, kinesio taping and dry needling. Studies have shown us that the conservative management of S.I. joint pain with physical therapy can have a significant effect on pain and disability.
Medicinal and Invasive Interventions
Medication
Medical management can include passive therapies like medications to help reduce the pain. NSAIDS and muscle relaxers are 2 that your Physician might prescribe you. While helpful they do not fix the root cause of the issue.
Injections
Corticosteroid injections are another route that your physician can suggest to address pain. These are small procedures where they inject a steroid directly to the S.I. joint to reduce the pain. This video does a great job of describing the procedure. There are a number of ways that your physician might inject the medication but that would be based on their clinical decision making and your specific presentation. Steroid injections are often a second line of defense when conservative management was not effective or in conjunction with physical therapy so that you can get the most out of it . Studies like this one have shown that injections after conservative management has failed can be very effective in reducing pain, helping people return to work and reducing their need for medication use.
Radiofrequency Ablation
This is an “newer” procedure being implemented by Physicians as another nonsurgical intervention for S.I. joint pain. It used to heat the nerves in order to interrupt pain signals to spinal nerves and thus reduce the sensation of pain. Due to the fact that the procedure has not been around for too long, research is still limited in its effectiveness. A systematic review comparing a large group of studies found that over all, radiofrequency ablation of S.I. joint pain does not seem to make a significant effect on pain in the long term but can have small effects in the short term.
Surgery
The most invasive option for managing this condition would be a surgical Intervention, most likely a fusion of the S.I. joint. This is where anchors are placed across the joint in order to stabilize it and minimize any excessive movement. This is usually the last option that is explored and usually due to failure of all previous interventions. A study which followed 52 patients undergoing S.I. joint fusion found positive outcomes after surgery in pain, disability and quality of life 1 year after surgery. This procedure can be helpful but it is so important to remember that surgery is a big deal and major change to your body which comes with its own sets of risks. We highly encourage clients to give conservative management a good shot before considering surgery but this all under guidance of your physician.
When should you do something about it?
Now! Be encouraged that there are so many options out there for you in order to tackle this pain head on. The problem with letting pain like this linger is that it starts to alter how our body interprets that pain and it becomes much more sensitive and irritable. This then leads to higher disability, higher pain and affects your quality of life. This video explains this concept in a little more detail with examples that we all can relate to. Whether this pain is old or new, go get help so you can get back to your pain free life!
References:
Al-Subahi, M., Alayat, M., Alshehri, M. A., Helal, O., Alhasan, H., Alalawi, A., … & Alfaqeh, A. (2017). The effectiveness of physiotherapy interventions for sacroiliac joint dysfunction: a systematic review. Journal of physical therapy science, 29(9), 1689-1694.
Domenico Prestamburgo, M. D., Paolo Gaetani, M. D., & Daniel Cher, M. D. (2017). 1-year results of a randomized controlled trial of conservative management vs. minimally invasive surgical treatment for sacroiliac joint pain. Pain Physician, 20, 537-550.
Eno, J. J. T., Boone, C. R., Bellino, M. J., & Bishop, J. A. (2015). The prevalence of sacroiliac joint degeneration in asymptomatic adults. JBJS, 97(11), 932-936
Leggett, L. E., Soril, L. J., Lorenzetti, D. L., Noseworthy, T., Steadman, R., Tiwana, S., & Clement, F. (2014). Radiofrequency ablation for chronic low back pain: a systematic review of randomized controlled trials. Pain Research and Management, 19(5), e146-e153.
Slipman, C. W., Lipetz, J. S., Plastaras, C. T., Jackson, H. B., Vresilovic, E. J., Lenrow, D. A., & Braverman, D. L. (2001). Fluoroscopically guided therapeutic sacroiliac joint injections for sacroiliac joint syndrome. American journal of physical medicine & rehabilitation, 80(6), 425-432.
{kind=link}
{kind=link}
{kind=link}